Environmental Sensitivities as a Public Health and Disability Issue: ANRES Data Analysis 2015–2025
Evidence, Multimorbidity, Lived Impacts, and the Case for Disability Recognition
By Dr Sharyn Martin
https://anres.org/wp-content/uploads/2026/06/ANRES-2026-Report-PDF.docx.pdf
Table of Contents
1.1 Main Hardships Faced by People with Environmental Sensitivities.
Section 2.0 Environmental Sensitivity (ES) Conditions Selected.
2.1 Environmental Sensitivity Conditions Selected by Registrants.
2.2 Environmental Sensitivity Conditions by Gender
2.3 Other Co-Existing Non-ES Medical Conditions/Diseases.
2.4 Number of concurrent Conditions Selected.
2.5 Number of concurrent conditions by Gender
2.6 One Environmental Sensitivity Condition Selected.
2.7 Characteristics of Environmental Sensitivities Registrants.
2.7.1 Age of Current Registrants.
2.7.2 Age at Onset of Environmental Sensitivity Conditions.
2.7.3 Gender Difference in Age at Which Condition/s Developed.
2.7.4 Duration with Environmental Sensitivity Conditions.
2.8 Features Environmental Sensitivities Share.
2.9 Possible Contributing Factors.
Section 3.0 Common Environmental Sensitivity Co-conditions.
3.1 Summary: Common Environmental Sensitivity Co‑conditions.
Section 4.0 Hardships and Challenges Associated with Environmental Sensitivities.
4.2 Hardships Faced by Individuals with Environmental Sensitivities.
4.2.1 Number of Concurrent Hardships.
4.2.2 Additional Hardships Reported.
Section 5.0 The Consequences of Environmental Illnesses.
5.1 Impact, Burden, and Disability Consequences.
5.2 Living Adjustments and Financial Burden.
5.3 Barriers to Healthcare and Support Services.
5.4 Social Exclusion, Identity Loss, and Disability Progression.
5.5 Summary: Environmental Illness as a Disability Issue.
6.1 Environmental Sensitivities as Multisystem and Multimorbid Conditions.
6.2 Gender, Age, and Cumulative Impact
6.3 Disability Is Shaped by Environment, Not Just Illness.
6.4 Healthcare Inaccessibility as a Driver of Harm..
6.5 Implications for Policy, Services, and Disability Recognition.
6.6 Strengths, Limitations, and Future Directions.
Appendix: Advocacy Statement on Environmental Sensitivities.
Environmental Sensitivities Are a Disability—Recognition Is Long Overdue.
1. Formal Recognition of Environmental Sensitivities as Disabilities.
2. Ending Invisibility Through Public Awareness.
3. Safe, Accessible Housing Is a Human Right
4. Healthcare Access Without Harm.
5. Employment With Dignity and Accommodation.
6. Education Without Exclusion.
7. Public Spaces Must Be Accessible to All
8. Social Services That Understand and Respond.
1. Public Education and Advocacy Campaigns.
2. Healthcare Training and Accountability.
3. Policy Reform and Legislative Action.
4. Community‑Led Support and Empowerment
6. Safe Housing: Practical, Proven Solutions.
Opening Statement
Imagine being excluded from housing, healthcare, work, education, and public life—not because of choice, but because the environments around you cause harm.
For individuals with Environmental Sensitivities, this exclusion is not hypothetical. It is lived reality.
Recognition, accommodation, and inclusion are not special treatment—they are fundamental rights. Addressing Environmental Sensitivities is a matter of equity, dignity, and justice. The time for action is now.
Summary
The ANRES 2025 Report analyses data from the Australian National Register of Environmental Sensitivities (ANRES) collected between 2015 and 2025, based on responses from 553 individuals aged 4 to 95 years. The findings provide strong evidence that Environmental Sensitivities (ES)—including Multiple Chemical Sensitivity (MCS), Fragrance sensitivity, Food sensitivity, Electromagnetic Hypersensitivity (EHS), Chronic Fatigue Syndrome/ Myalgic Encephalomyelitis (CFS/ME), Fibromyalgia, Lyme disease, and Biotoxin‑related illness—are chronic, disabling, and highly co‑occurring conditions with substantial impacts on daily functioning and quality of life.
The data show that Environmental Sensitivities rarely occur in isolation. Most registrants reported multiple conditions, long illness duration, and significant cumulative impairment. Females were disproportionately affected and more likely to experience higher levels of multimorbidity. Onset commonly occurred in early to mid‑adulthood, with many individuals living with these conditions for decades, highlighting their long‑term and progressive nature.
Registrants reported widespread environmental barriers to healthcare, housing, employment, education, and access to public and community spaces. Exposure to fragrances, chemicals, mould, and electromagnetic fields in everyday environments—including medical facilities, workplaces, schools, public transport, and housing—frequently prevents safe access to places that provide essential services. These barriers contribute to social isolation, financial hardship, psychological distress, and loss of independence, with employment disruption and difficulty accessing appropriate healthcare among the most severe impacts.
The report concludes that Environmental Sensitivities represent a significant but under‑recognised public health and disability issue in Australia. The lack of formal recognition and accommodation exacerbates exclusion and prevents access to disability supports and protective policies. The report calls for urgent systemic action, including formal disability recognition, improved professional awareness, and practical environmental accommodations across healthcare, housing, employment, education, and public infrastructure to uphold equity, dignity, and human rights.
Section 1.0 Introduction
Environmental Sensitivities (ES) refer to a collection of chronic conditions where individuals experience adverse reactions to chemicals, perfumes, moulds, electromagnetic fields, and other environmental factors at levels that are generally tolerated by the wider population. This study aimed to explore the intersection of these Environmental Sensitivity conditions and the everyday challenges faced by those living with what are largely invisible disabilities.
The report highlights the unique difficulties met by people of varying ages. Young individuals may struggle in school environments due to the prevalence of fragrances used by both peers and staff, or where parents of school aged children have Environmental Sensitivities themselves and have difficulties attending school activities such as parent-teacher meetings, while older adults might find it challenging to access essential community resources and healthcare facilities because of their sensitivities.
Environmental Sensitivities discussed in this report are predominantly hidden or invisible disabilities within society. These include Multiple Chemical Sensitivity (MCS), Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME), Lyme disease, Biotoxin-related Illnesses, Fibromyalgia, Electromagnetic Hypersensitivity (EHS), as well as Fragrance and Food Sensitivities.
If left undiagnosed or without proper treatment, Environmental Sensitivities can have far-reaching consequences. These conditions affect not only the individual’s health, but also influence lifestyle, family dynamics, and financial security. Those affected may face considerable obstacles in securing employment, accessing social and health services, supporting themselves and their families, socialising, pursuing education, and using public amenities like hospitals, schools, libraries, shopping centres, public toilets and healthcare facilities.
Many individuals endure significant hardships and are frequently overlooked—often due to the absence of formal recognition or evidence of their condition. Some sufferers are still undiagnosed and are unaware that environmental factors contribute to their poor health. Continued exposure to triggers may further heighten their sensitivities as time goes on.
Recognising Environmental Sensitivity conditions as legitimate medical disabilities is crucial. Such acknowledgement enables the implementation of practical measures, including the provision of safer housing, increased employment opportunities, financial assistance, better educational settings, and improved access to medical and disability services. Raising awareness and visibility of Environmental Sensitivities is fundamental to starting meaningful changes in the lives of those living with these hidden disabilities.
In many situations, individuals are left financially vulnerable, with some relying on disability pensions that are insufficient to cover the cost of necessary medical aids, nutritional supplements, organic or specialised foods or assistance needed for a reasonable quality of life.
1.1 Main Hardships Faced by People with Environmental Sensitivities
- Access to Medical Assistance: 67.0% report difficulties in obtaining proper healthcare services.
- Securing Safe and Affordable Housing: 52.3% struggle to find suitable living environments.
- Obtaining Education: 35.0% face barriers in attending educational institutions.
- Gaining and Maintaining Employment: 76.8% encounter challenges in securing work or generating income.
- Accessing Social Services Safely: 34.5% have trouble accessing necessary social services.
- Public Space Access: 67.9% experience difficulties entering public spaces such as workplaces and schools.
- Maintaining Relationships and Social Interaction: 83.7% report problems with personal relationships and social engagement.
These difficulties contribute to increased social isolation and economic disadvantage, making it even more challenging for affected individuals to keep relationships, secure stable housing, and achieve financial security.
The study also proves that people with Environmental Sensitivities often experience a range of co-morbid conditions, leading to severe impairments. These conditions can result in substantial disabilities and hardships across many areas of daily life, including physical health, employment, and social relationships.
Overall, the findings emphasise the broad and pervasive impact of Environmental Sensitivities on affected individuals. There is a significant need for recognition, understanding, and support to improve the quality of life and access to essential services for this population. Addressing these challenges will require coordinated action from healthcare providers, policymakers, and the wider community to foster a more inclusive environment for people with Environmental Sensitivities. A shift in attitudes, beliefs, and actions regarding health and the environment is necessary to improve health outcomes for individuals and communities.
This report strongly advocates for recognising Environmental Sensitivities as disabilities, to facilitate better access to housing, employment, and medical services. Furthermore, it underscores the importance of societal awareness and understanding of these invisible disabilities, which are often not recognised by the health system or the public.
The appendices to this document contain recommendations and strategies to address the lack of recognition and support for people with Environmental Sensitivities.
Section 2.0 Environmental Sensitivity (ES) Conditions Selected
Data were collected and analysed from registrations on the Australian National Register of Environmental Sensitivities (ANRES) website (www.anres.org) between 2015 and 2025. Registrants were able to select one or more Environmental Sensitivity (ES) condition/s, including Multiple Chemical Sensitivity (MCS), Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME), Electromagnetic Hypersensitivity Syndrome (EHS), Fragrance Sensitivity, Food Sensitivity, Fibromyalgia, Lyme disease and/or co‑infections, Biotoxin‑related illness, and other medical conditions.
2.1 Environmental Sensitivity Conditions Selected by Registrants
The most often reported conditions were MCS, Fragrance Sensitivity, and Food Sensitivity, followed by EHS, Chronic Fatigue Syndrome/Myalgic Encephalomyelitis CFS/ME, and Fibromyalgia (Table 1). Although fewer registrants reported Lyme disease or Biotoxin‑related illness, strong associations with MCS were found. Of those reporting Biotoxin‑related illness, 95.7% also reported MCS, while 78.0% of those reporting Lyme disease also had MCS.
Table 1 presents the number and percentage of registrants selecting each Environmental Sensitivity condition. Many registrants reported multiple conditions, highlighting the complex and overlapping nature of Environmental Sensitivities.
Table 1. Environmental Sensitivity Conditions Selected
| Environmental Sensitivity Conditions | Number | Percentage % |
| MCS | 411 | 77.1 |
| Fragrance Sensitivity | 407 | 76.4 |
| EHS | 246 | 46.2 |
| Food Sensitivity | 368 | 69.0 |
| CFS/ME | 231 | 43.3 |
| Fibromyalgia | 149 | 28.0 |
| Lyme Disease &/or its co-infections | 50 | 9.4 |
| Biotoxin-related illness | 46 | 8.6 |
| Other conditions/aliments | 144 | 27.0 |
Table 1. Number and percentage of respondents selecting each Environmental Sensitivity condition. Respondents were able to select more than one condition; therefore, percentages do not sum to 100%.
2.2 Environmental Sensitivity Conditions by Gender
Of the 553 registrants, 446 (83.7%) were female and 86 (16.1%) were male. Analysis by gender (Table 2) shows that females reported higher prevalence across most Environmental Sensitivity conditions, including MCS, Fragrance Sensitivity, Food Sensitivity, CFS/ME, Fibromyalgia, Lyme disease, and Biotoxin‑related illness. Males reported slightly higher prevalence of EHS. Both the percentage of females with MCS (80%) and Fragrance Sensitivity (79.8%) were significantly higher than males (61.9%) with MCS and (58.1%) with Fragrance Sensitivity.
The proportion reporting other non‑specified conditions was similar between males (25.6%) and females (27.4%). Overall, females were more likely to report a greater number of co‑existing conditions.
Molot (2013) found that women are affected by more Environmental Sensitivity conditions than males. Molot (2013) found Environmental Sensitivity conditions are more common in women because women are more responsive to their environment via both limbic and immune systems, have a greater burden of chemical exposures and less efficient detoxification systems compared to men.
Table 2. Gender vs Conditions
| Environmental Sensitivity Conditions by Gender | ||||
| Environmental Sensitivity Conditions | Males (n= 86) | Female (n= 446) | ||
| Number | Percentage (%) | Number | Percentage (%) | |
| MCS | 53 | 61.9% | 357 | 80.0% |
| Fragrance Sensitivity | 50 | 58.1% | 356 | 79.8% |
| EHS | 46 | 53.5% | 199 | 44.6% |
| Food Sensitivity | 47 | 54.7% | 320 | 71.7% |
| CFS/ME | 30 | 34.9% | 201 | 45.1% |
| Fibromyalgia | 11 | 12.8% | 138 | 30.9% |
| Lyme Disease &/or its co-infections | 8 | 9.3% | 42 | 9.4% |
| Biotoxin-related illness | 4 | 4.7% | 42 | 9.4% |
| Other | 22 | 25.6% | 125 | 27.4% |
Table 2. Number and percentage of male and female respondents reporting each Environmental Sensitivity condition.
2.3 Other Co-Existing Non-ES Medical Conditions/Diseases
Registrants often reported additional medical conditions alongside Environmental Sensitivities. These included Ehlers‑Danlos Syndrome (hypermobile type), Mast Cell Activation Syndrome (MCAS), Chronic Inflammatory Response Syndrome (CIRS), autoimmune diseases, allergies, neurological disorders, respiratory diseases (including asthma and COPD), and sensory sensitivities to noise and light.
MCAS and Ehlers‑Danlos Syndrome were commonly reported, indicating notable overlap with Environmental Sensitivities. Several registrants without a specific Environmental Sensitivities (ES) diagnosis reported symptoms consistent with chemical sensitivity or neurological dysfunction, such as temporomandibular joint disorder, occipital neuralgia, dizziness, fatigue, and sensitivity to smoke or food preservatives.
- Ehlers-Danlos Syndrome (Hypermobile): This condition is mentioned multiple times, indicating its prevalence among the listed conditions. Ehlers-Danlos Syndrome (EDS) is a group of connective tissue disorders characterised by various symptoms, primarily affecting the skin, joints, and blood vessel walls.
- Mast Cell Activation Syndrome (MCAS): This is another frequently cited condition, highlighting its significance. Mast Cell Activation Syndrome (MCAS) is a condition characterised by inappropriate and excessive release of chemicals such as histamine from mast cells, leading to a variety of dermatological, gastrointestinal, respiratory and cardiovascular symptoms.
- Chronic Inflammatory Response Syndrome (CIRS): This condition appears several times, suggesting its common occurrence. Chronic inflammatory response syndrome is a multisystem and multi-symptom illness that occurs when a person gets exposed to toxins such as mould spores or biotoxins found in tick or spider bites. These toxins get attached to the immune system to trigger an inflammatory response and induce hormonal changes. The immune system produces an excess of cytokines that can lead to the immune system attacking its tissues, causing inflammation and other associated symptoms.
- Autoimmune diseases: Various autoimmune conditions are mentioned, reflecting their widespread impact.
- Allergies: Several types of allergies, including food allergies and sensitivities to environmental factors, are commonly mentioned.
- Noise and light sensitivities: These sensitivities are repeatedly cited, indicating their importance.
- Neurological Disease:cognitive, motor and sensory disorders and peripheral nervous system disorders
- Respiratory Disease; Including asthma and chronic obstructive pulmonary disease (COPD)
2.4 Number of concurrent ES Conditions Selected
Registrants were able to select multiple Environmental Sensitivity conditions. Most individuals reported between three and five conditions, with nearly one quarter reporting four conditions (Table 3). This demonstrates a high degree of co‑morbidity among individuals with Environmental Sensitivities.
Table 3. Number of concurrent conditions per person
| Number of Environmental Sensitivity Conditions | ||
| Conditions | Number | Percentage % |
| 0 | 4 | 0.8 |
| 1 | 56 | 10.8 |
| 2 | 79 | 15.2 |
| 3 | 104 | 20.0 |
| 4 | 128 | 24.7 |
| 5 | 82 | 15.8 |
| 6 | 11 | 9.8 |
| 7 | 4 | 2.1 |
| 8 | 4 | 0.8 |
Table 3. Distribution of the number and percentage of Environmental Sensitivity conditions reported per respondent.
Analysis by age group (Table 4) shows that individuals aged 61 years and over were more likely to report a higher number of conditions, particularly four or more. This suggests cumulative effects of environmental exposures and long‑term illness over time.
Table 4. Number of concurrent conditions and age groups
| Age group | Number with 1-3 conditions | Percent of 1-3 condition % | Number with 4-6 conditions | Percent of 4-6 conditions % | Number with 7-8 conditions | Percent 7-8 conditions % |
| 0-15 | 1 | 0.4 | 0 | 0.0 | 0 | 0.0 |
| 16-30 | 5 | 2.9 | 4 | 3.0 | 1 | 5.5 |
| 31-45 | 22 | 9.2 | 18 | 4.5 | 2 | 11.0 |
| 46-60 | 91 | 31.3 | 52 | 13.5 | 8 | 44.4 |
| 61+ | 120 | 50.2 | 59 | 44.3 | 7 | 38.9 |
Table 4. Number and percentage of respondents within each age group reporting one to three, four to six, or seven to eight Environmental Sensitivity conditions.
2.5 Number of concurrent conditions by Gender
Table 5. Difference between gender number of conditions
| Number of conditions | Male n = 86 | Female n = 446 | ||
| Number | Percentage | Number | Percentage | |
| 1 | 17 | 19.8% | 39 | 8.7% |
| 2 | 19 | 22.1% | 60 | 13.5% |
| 3 | 14 | 16.3% | 90 | 20.2% |
| 4 | 15 | 17.4% | 112 | 25.1% |
| 5 | 8 | 9.3% | 74 | 16.6% |
| 6 | 5 | 5.8% | 46 | 10.3% |
| 7 | 0 | 0.0% | 11 | 2.5% |
| 8 | 0 | 0.0% | 4 | 0.9% |
| 1-3 conditions | 50 | 58.1% | 189 | 42.4% |
| 4-8 conditions | 28 | 32.6% | 247 | 55.4% |
Table 5. Number and percentage of male and female respondents reporting one to three or four to eight Environmental Sensitivity conditions.
Females were more likely to report four or more conditions (55.4%), whereas males were more likely to report one to three conditions (58.1%) (Table 5). This further supports the finding that Environmental Sensitivities tend to be more complex and multi‑system in females.
2.6 One Environmental Sensitivity Condition Selected
Only 55 registrants (10.5%) reported a single Environmental Sensitivity condition. EHS accounted for most of these cases (5.4%) (Table 6).
Individuals reporting EHS alone commonly associated the onset of their condition with increased exposure to wireless technologies, including mobile phones, Wi‑Fi, smart meters, and mobile phone towers. Many reported significant restrictions in daily activities, including limited access to public spaces such as medical facilities, shopping centres, and libraries.
Table 6. Number of registrants with one Environmental Sensitivity Condition
| Environmental Sensitivity Conditions | Number | Percentage % |
| MCS | 4 | 1.9 |
| Fragrance Sensitivity | 8 | 1.5 |
| EHS | 29 | 5.4 |
| Food Sensitivity | 1 | 0.2 |
| CFS/ME | 3 | 0.6 |
| Fibromyalgia | 0 | 0.0 |
| Lyme Disease &/or its co-infections | 1 | 0.2 |
| Biotoxin-related illness | 0 | 0.0 |
| Other conditions/aliments | 4 | 0.8 |
Table 6. Number and percentage of respondents reporting only one Environmental Sensitivity condition, by condition type.
2.7 Characteristics of Environmental Sensitivities Registrants
Age, onset and duration of Environmental Sensitivities
2.7.1 Age of Current Registrants
The ANRES database includes 553 registrants aged between 4 and 95 years. Of the 553 there are 446 (83.7%) females, and 86 (16.1%) males. These numbers are consistent with overseas and Australian estimates of 80% women compared to 20% in men (Caress & Steinmann 2003; NSW Public Health 2002; Fitzgerald 2008).
68.3 % of registrants have a formal a diagnosis of one or more conditions and 31.7% with no formal diagnosis. The undiagnosed condition/s were self-diagnosis or diagnosed by a non-medical health practitioner.
Most registrants were aged between 46 and 60 years, followed closely by those aged 61 years and over (Table 7).
Table 7. Current Age Distribution of Registrants
| Current Age Groups of Registrants | ||
| Age group | Number | Percentage (%) |
| 0-15 | 3 | 0.6 |
| 16-30 | 18 | 3.4 |
| 31-45 | 56 | 10.5 |
| 46-60 | 215 | 40.4 |
| 61+ | 240 | 45.1 |
Table 7. Number and percentage of respondents by current age group at the time of registration.
2.7.2 Age at Onset of Environmental Sensitivity Conditions
The age at which their Environmental Sensitivity condition developed was collected from 436 of the 533 (81.8 %) registrants who were able to provide a year when their sensitivity/s started.
Table 8. Age at Onset of Environmental Sensitivity Conditions
| Age when developed Environmental Sensitivities | ||
| Age when developed | Number | Percentage (%) |
| 0-10 | 38 | 8.7 |
| 10-20 | 30 | 6.9 |
| 20-30 | 86 | 19.7 |
| 30-40 | 99 | 22.7 |
| 40-50 | 112 | 25.6 |
| 50-60 | 52 | 11.9 |
| 60+ | 19 | 4.3 |
Table 8. Number and percentage of respondents by age group at which Environmental Sensitivity conditions were reported to have first developed.
The minimum age when Environmental Sensitivities began was from birth to a maximum age of 76 years. The average age was 36.6 years. Many people were aged between 20-50 years when their condition/s developed with a Mode of 50 years and Median of 37 years.
Environmental Sensitivities can develop at any age (Shannon et al 2003; Wolf, 2000 and increase with age (Sears, 2007). The majority of registrants are 45-64 years, consistent with those in the Halapy and Parlour’s (2013) study.
2.7.3 Gender Difference in Age at Which Condition/s Developed.
Table 9. Gender Differences in Age at Onset of Environmental Sensitivity Conditions
| Gender Differences in Age of Onset of Environmental Sensitivity Conditions | ||||
| Age at which condition developed | Males | Females | ||
| Number | Percent % | Number | Percent % | |
| 0-10 | 8 | 11.3% | 30 | 11.3% |
| 11-20 | 3 | 4.2% | 27 | 7.4% |
| 21-30 | 15 | 21.1% | 71 | 19.5% |
| 31-40 | 20 | 28.2% | 79 | 21.7% |
| 41-50 | 13 | 18.3% | 99 | 27.2% |
| 51-60 | 5 | 7.0% | 47 | 12.9% |
| 61+ | 7 | 9.9% | 11 | 3.0% |
Table 9. Number and percentage of male and female respondents by age group at which Environmental Sensitivity conditions developed.
There is minor difference in the age between the sexes as to when their condition developed.
2.7.4 Duration with Environmental Sensitivity Conditions
Data on age of onset were available for 82.2% of registrants. Environmental Sensitivities most developed between 20 and 50 years of age, with an average onset age of 36.6 years (Table 8). There were minimal differences between males and females in age of onset (Table 9).
The average duration of illness was 23.1 years, with over half of registrants living with their condition(s) for more than 16 years (Table 10).
Of the 438 (82.2%) who knew when their condition starts the average number of years is 23.1, minimum 1 maximum 84.
The age when condition developed was similar between the genders, 30.4 years for females and 34.5 years for males.
Table 10. Duration Living with Environmental Sensitivity Conditions
| Duration (years) with the Conditions/s | ||
| Duration with the Condition/s | Number | Percentage (%) |
| 0-5 | 11 | 2.5 |
| 6-10 years | 66 | 15.0 |
| 11-15 years | 118 | 26.9 |
| 16+ | 243 | 55.4 |
Table 10. Number and percentage of respondents by duration (years) living with Environmental Sensitivity conditions.
2.8 Features Environmental Sensitivities Share
The characteristics commonly associated with Environmental Sensitivity conditions include their chronicity, environmental triggers, and frequent coexistence with other long-term co-morbidities. These conditions impact the nervous system as well as various organs and bodily systems.
With increasing severity, the likelihood of additional co-morbidities rises, resulting in many individuals presenting with two or more conditions concurrently. Each of these disorders has the potential to produce severe symptoms and, in advanced cases, lead to complete disability (Halapy & Parlour 2013). This trend was demonstrated in Halapy and Parlour’s (2013) study, which found that registrants often developed co-morbid conditions over a span of several years.
In addition to these physical health challenges, immune system dysfunction is a prominent feature of such conditions. Many individuals with Environmental Sensitivities exhibit impaired detoxification mechanisms that are susceptible to being overwhelmed by excessive oxidative stress (Stein & Udasin 2020).
Furthermore, Environmental Sensitivities are frequently accompanied by significant social barriers. These conditions are frequently described as ‘invisible’. Many affected individuals deliberately isolate themselves from the community to avoid toxic exposures and lack of understanding. Consequently, they are removed from public visibility and, therefore, more easily overlooked. For instance, an ASEHA survey conducted in 2011 reported that nearly 90% of individuals with Multiple Chemical Sensitivity lived in a state of high or medium isolation (ASEHA 2011).
Moreover, individuals with these conditions often do not display visible markers of disability, such as the use of wheelchairs. The absence of overt physical indicators, combined with a lack of diagnostic clarity or recognition in mainstream medical practice, and scepticism from the broader public, contributes to the persistent lack of awareness surrounding these invisible illnesses. This widespread lack of awareness frequently results in disbelief and inadequate support for affected individuals.
2.9 Possible Contributing Factors
Several key factors may be contributing to the development of Environmental Sensitivity conditions and their consequential chronic health issues. These include:
- Diet: Consuming substantial amounts of fried and highly processed foods, as well as products containing pesticide residues, preservatives, and artificial colours, can place a burden on the body’s metabolic processes and increase the risk of long-term health problems.
- Exposure to toxins: Contact with harmful substances in food, water, air, and through skin—such as heavy metals, pesticides, and industrial chemicals—can disrupt cellular processes, damage organs, and negatively affect overall health.
- Constant mental stress: Ongoing stress from work, social pressures, or personal challenges can impair immune function, disrupt hormonal balance, and contribute to chronic illness.
- Sedentary lifestyle and demanding work schedules: Lack of physical activity combined with busy, high-pressure routines leads to weakened cardiovascular health, poor muscle tone, and increased susceptibility to disease.
- Microbial infection: Exposure to infectious microbes that breach the body’s physical barriers, especially when the immune system is compromised, may result in chronic immune dysfunction and persistent health complications.
- Genetic susceptibility. These variations may influence the proteins involved in the immunological response, detoxification, metabolic processes, and how genes express themselves (DeLuca et al. 2010). Genetic variants related to phase I and phase II detoxification of xenobiotic compounds are linked to multiple chemical sensitivity. (Moon 2026)
- Phenotype Disease Network where diseases may be interconnected through shared phenotypes, where one condition increases susceptibility to others.
- Environmental exposures to substances such as mould, EMR and chemicals. These substances can interact leading to additive or synergistic effects that complicate health risk assessments. (Ledoigt et al. 2015)
- Environmental diseases are often late-onset, developing after decades of exposure. Mechanisms contributing to this breakdown include:
- Oxidative Stress: Damage caused by reactive oxygen species.
- Epigenetic Effects: Alterations in gene expression due to environmental factors.
- Inflammation: Chronic inflammation leading to tissue damage.
- Endocrine Disruption: Interference with hormonal systems. (Zeliger 2014)
These factors often work together, amplifying their effects and increasing the risk of chronic health problems.
Section 3.0 Common Environmental Sensitivity Co-conditions
Evidence is mounting that Environmental Sensitivity (ES) conditions are associated with immune and inflammatory dysregulation, altered neurotransmitter signalling, microbiome perturbations, and metabolic and mitochondrial abnormalities (Hu & Baines 2018). Genuis (2014) describes a related framework—toxicant‑induced loss of tolerance—as a possible mechanism through which repeated or cumulative exposures contribute to the development of multiple, overlapping chronic conditions. In this context, Environmental Sensitivities is frequently characterised by multimorbidity, with two or more ongoing conditions occurring within the same individual (Genuis 2014).
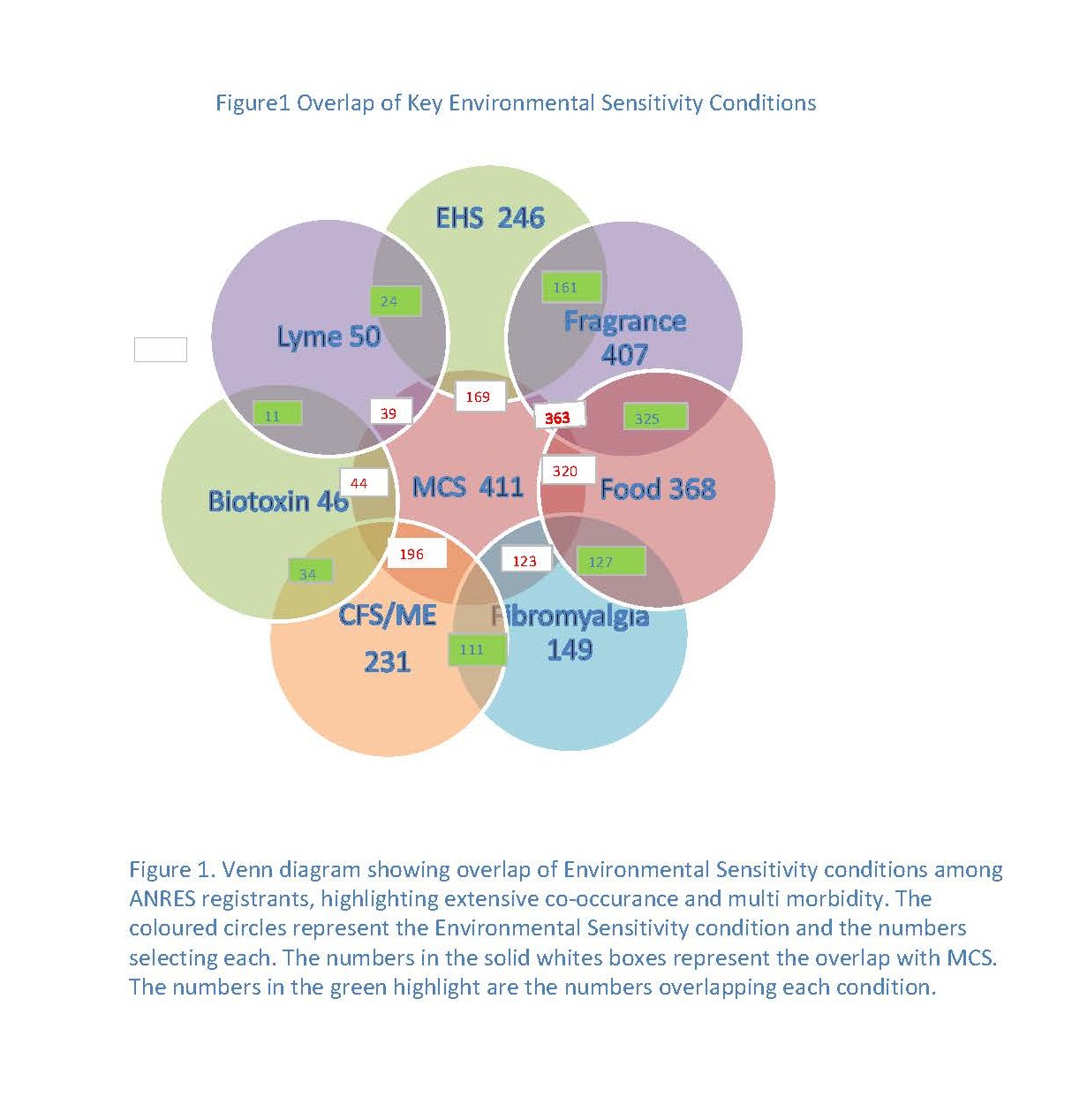
To describe this multimorbidity, we analysed overlap between pairs of Environmental Sensitivity conditions. The resulting co‑condition patterns are summarised in Tables 11 to 19 and Figure 1. Venn diagram, figure 1. shows the visual relationships between the Environmental Sensitivity conditions
Across the dataset, Multiple Chemical Sensitivity (MCS), Fragrance Sensitivity, and Food Sensitivity were the most frequently reported and most consistently co‑occurring conditions. As a result, environmental accommodations designed to support people with MCS (e.g., fragrance‑free and low‑chemical practices in buildings and public/outdoor spaces) are likely to benefit a broad proportion of people living with Environmental Sensitivities.
This section also highlights how often Environmental Sensitivity conditions overlap—and why that overlap matters for policy, service access, and disability recognition. The ANRES data show a consistent pattern: people rarely live with one sensitivity in isolation. Instead, they experience clusters of conditions that compound symptoms, increase exposure risks, and intensify barriers to safe participation in everyday life. In practical terms, this overlap means that a single accommodation (for example, fragrance-free and low-chemical practices) can reduce harm for many people at once—and that failing to provide these accommodations can exclude people from multiple essential settings simultaneously (healthcare, workplaces, education, housing, and community services).
Table 11 Environmental Sensitivities Conditions Overlap
| Environmental Sensitivities Conditions overlaps. | ||||||||
| Environmental Sensitivity Conditions | Co-conditions (percentage (%) of those with the condition) | |||||||
| MCS | CFS | EHS | Fibromyalgia | Fragrance sensitivity | Food Sensitivity | Biotoxin | Lyme | |
| MCS | — | 84.8 | 68.7 | 82.6 | 89.2 | 87.0 | 95.7 | 78.0 |
| CFS | 47.7 | — | 40.7 | 74.5 | 47.9 | 51.9 | 73.9 | 76.0 |
| Fibromyalgia | 29.9 | 48.1 | 24.4 | — | 32.2 | 34.5 | 43.5 | 40.0 |
| Fragrance Sensitivity | 88.3 | 84.4 | 65.4 | 82.6 | — | 88.3 | 78.3 | 76.0 |
| EHS | 41.1 | 43.3 | — | 40.3 | 39.6 | 46.7 | 60.9 | 48.0 |
| Food Sensitivity | 79.9 | 82.7 | 69.9 | 85.2 | 79.9 | —- | 76.9 | 76.0 |
| Biotoxin | 10.7 | 14.7 | 11.4 | 13.4 | 8.8 | 9.2 | 23.9 | — |
| Lyme Disease | 9.5 | 16.5 | 9.8 | 13.4 | 9.3 | 10.3 | —- | 22.0 |
Table 11. Percentage overlap of co-conditions among individuals with Environmental Sensitivity conditions. Values represent the proportion (%) of respondents with a given primary condition who also reported each listed co-condition. The numbers in red represent the largest percentages of respondents.
Table 12. MCS and co-conditions
| MCS and Co-Conditions | ||
| Co-conditions | Number | Percent % |
| EHS | 169 | 41.1% |
| CFS/ME | 196 | 47.7% |
| Food Sensitivities | 320 | 77.9% |
| Fragrance Sensitivities | 363 | 88.3% |
| Fibromyalgia | 123 | 29.9% |
| Other Condition | 104 | 25.3% |
| Biotoxin-related illness | 44 | 10.7% |
| Lyme Disease &/or its co-infections | 39 | 9.5% |
| MCS alone | 10 | 2.4% |
Table 12. Frequency and percentage distribution of co-occurring conditions reported by respondents with Multiple Chemical Sensitivity (MCS) Percentages represent the proportion of individuals with MCS reporting each co-condition. The numbers in red represent the largest percentages of respondents.
Table 13. Food Sensitivity and Co-conditions
| Food Sensitivity and Co-conditions | ||
| Co-conditions | Number | Percent % |
| MCS | 320 | 87.0% |
| CFS/ME | 191 | 51.9% |
| EHS | 172 | 46.7% |
| Fragrance Sensitivity | 325 | 88.3% |
| Fibromyalgia | 127 | 34.5% |
| Food Sensitivity alone | 1 | 0.3% |
| Other Condition | 107 | 29.1% |
| Biotoxin-related illness | 34 | 9.2% |
| Lyme Disease &/or its co-infections | 38 | 10.3% |
Table 13. Frequency and percentage respondents with Food Sensitivity reporting co-existing Environmental Sensitivity-related conditions. Percentages are calculated within the Food Sensitivity cohort. The numbers in red represent the largest percentages of respondents.
Table 14. Fragrance Sensitivity and Co-conditions.
| Fragrance and Co-conditions | ||
| Co-conditions | Number | Percent % |
| MCS | 363 | 89.2% |
| CFS/ME | 195 | 47.9% |
| EHS | 161 | 39.6% |
| Fibromyalgia | 131 | 32.2 |
| Food Sensitivity | 325 | 79.9 |
| Fragrance Sensitivity alone | 8 | 2.0 |
| Other Condition | 118 | 29.0 |
| Biotoxin-related illness | 36 | 8.8 |
| Lyme Disease &/or its co-infections | 38 | 9.3 |
Table 14. Prevalence of co-conditions among respondents reporting Fragrance Sensitivity. Values represent the percentage of individuals with Fragrance Sensitivity who also reported each listed condition. The numbers in red represent the largest percentages of respondents.
Table 15. Lyme Disease and Co-conditions
| L yme Disease and Co-conditions | ||
| Co-conditions | Number | Percent % |
| MCS | 39 | 78.0% |
| CFS/ME | 38 | 76.0% |
| EHS | 24 | 48.0% |
| Fibromyalgia | 20 | 40.0% |
| Fragrance Sensitivity | 38 | 76.0% |
| Food Sensitivity | 38 | 76.0% |
| Biotoxin-related illness | 11 | 22.0% |
| Lyme Disease alone | 1 | 2.0% |
| Other Condition | 12 | 24.0% |
Table 15. Distribution of co-occurring Environmental Sensitivity conditions among respondents reporting Lyme Disease and/or co-infections. Percentages reflect the proportion of the Lyme Disease subgroup. The numbers in red represent the largest percentages of respondents.
Table 16. Electromagnetic Hypersensitivity (EHS) and Co-conditions
| EHS and Co-conditions | |||
| Co-conditions | Number | Percent % | |
| CFS/ME | 100 | 40.7% | |
| Food sensitivities | 172 | 69.9% | |
| Fragrance Sensitivities | 161 | 65.4% | |
| Fibromyalgia | 60 | 24.4% | |
| MCS | 169 | 68.7% | |
| EHS alone | 29 | 11.8% | |
| Other Condition | 77 | 31.3% | |
| Biotoxin-related illness | 28 | 11.4% | |
| Lyme Disease &/or its co-infections | 24 | 9.8% | |
Table 16. Reported co-conditions among Electromagnetic Hypersensitivity respondents, expressed as number and percentage of respondents within the EHS cohort. The numbers in red represent the largest percentages of respondents.
Table 17. Chronic Fatigue Syndrome/Myalgic Encephalomyelitis CFS/ME
| CFS/ME and Co-conditions | ||
| Co-conditions | Number | Percent % |
| Fibromyalgia | 111 | 48.1% |
| Food Sensitivity | 191 | 82.7% |
| Fragrance Sensitivity | 195 | 84.4% |
| MCS | 196 | 84.8% |
| EHS | 100 | 43.3% |
| CFS alone | 3 | 1.3% |
| Other Condition | 67 | 29.0% |
| Biotoxin-related illness | 34 | 14.7% |
| Lyme Disease &/or its co-infections | 38 | 16.5% |
Table 17. Frequency and percentage of co‑occurring conditions reported by respondents with CFS/ME. Percentages represent the proportion of individuals with CFS/ME experiencing each co‑condition. The numbers in red represent the largest percentages of respondents.
Table 18. Fibromyalgia and Co-conditions
| Fibromyalgia and Co-conditions | ||
| Co-conditions | Number | Percent % |
| MCS | 123 | 82.6% |
| CFS/ME | 111 | 74.5% |
| EHS | 60 | 40.3% |
| Fragrance Sensitivity | 131 | 82.6% |
| Food Sensitivity | 127 | 85.2% |
| Fibromyalgia alone | 0 | — |
| Other Condition | 46 | 30.9% |
| Biotoxin-related illness | 20 | 13.4% |
| Lyme Disease &/or its co-infections | 20 | 13.4% |
Table 18. Prevalence of Environmental Sensitivity-related Co-conditions among respondents reporting Fibromyalgia. Percentages are calculated within the Fibromyalgia subgroup. The numbers in red represent the largest percentages of respondents.
Table 19. Biotoxin-Related Illness and Co-conditions
| Biotoxin and Co-conditions | ||
| Co-conditions | Number | Percent % |
| MCS | 44 | 95.7% |
| CFS/ME | 34 | 73.9% |
| EHS | 28 | 60.9% |
| Fibromyalgia | 20 | 43.5% |
| Fragrance Sensitivity | 36 | 78.3% |
| Food Sensitivity | 34 | 73.9% |
| Biotoxin alone | 0 | — |
| Lyme Disease &/or its co-infections | 11 | 23.9% |
| Other Condition | 12 | 26.1% |
Table 19. Number and percentage of respondents with Biotoxin-related illness reporting additional Environmental Sensitivity-related conditions. The numbers in red represent the largest percentages of respondents.
3.1 Summary: Common Environmental Sensitivity Co‑conditions
Environmental Sensitivities are not “minor sensitivities” or lifestyle preferences. They are complex, multi‑system health conditions that can be disabling—especially when everyday environments (air fresheners, fragrances, cleaning products, building emissions, mould, and electromagnetic exposures) are unavoidable. The growing evidence base points to interacting immunological, inflammatory, neurological, metabolic, and mitochondrial pathways that help explain why these conditions can be persistent, escalating, and difficult to manage without environmental controls.
The ANRES data make the real‑world implications clear: co‑occurrence is the norm. Multiple Chemical Sensitivity (MCS), Fragrance Sensitivity, and Food Sensitivity form a central cluster, frequently co‑existing with CFS/ME, Fibromyalgia, Electromagnetic Hypersensitivity (EHS), Lyme disease, and Biotoxin‑related illness. For service systems, this means people often face layered triggers and layered barriers—so piecemeal responses are not enough.
The overlap patterns also show how quickly disability can compound. People diagnosed with one Environmental Sensitivity condition are highly likely to experience multiple additional sensitivities, and those additional sensitivities can narrow access to safe housing, safe healthcare, and safe public participation. For example, most respondents with Biotoxin‑related illness or Lyme disease also reported MCS, while respondents with CFS/ME or Fibromyalgia frequently reported both fragrance and food sensitivities. These are not isolated “co‑morbidities”—they are cumulative burdens that require integrated care and practical environmental protections.
Taken together, the findings strengthen an urgent advocacy point: preventing exposure and reducing exposure is not optional—it is harm reduction. The data support the idea of toxicant‑induced loss of tolerance, where repeated or cumulative exposure can drive escalating intolerance and additional conditions over time (Miller CS,1999; Genuis 2010). This is exactly why recognition and accommodation matter: without safer environments, people may be forced into ongoing exposure that worsens health, increases disability, and deepens exclusion.
Section 4.0 Hardships and Challenges Associated with Environmental Sensitivities
Environmental Sensitivities (ES) drive exclusion—not because people “choose” to avoid places, but because many everyday environments are unsafe. Respondents described major barriers across healthcare, housing, employment, education, social participation, and financial security. These impacts are cumulative and often intensify with illness severity, duration, and the number of co‑existing conditions.
The most reported impacts—loss of employment or income, relationship strain, restricted access to public spaces, and inability to access appropriate medical care—are all markers of disability in practice. When people cannot safely enter clinics, workplaces, schools, or community services, the problem is not individual resilience; it is the lack of systemic accommodation.
Published research on the lived impacts of Environmental Sensitivities shows these conditions are pervasive and disabling, including loss of identity linked to contested recognition (Doiron 2007; Gibson et al. 1996; Gibson & Lindberg 2007; Gibson et al. 2005; Gibson et al. 1997; McCormick 2001; Zwillinger 1997; Gibson 2015); reduced income and disrupted work (Gibson and Lindberg 2007; Vierstra et al. 2007); impacts on social support (Gibson et al. 1998); barriers to medical care (Gibson et al. 2015); and restricted access to community resources (Gibson 2009; Gibson et al. 2011).
4.1 Age‑Related Impacts
Environmental Sensitivities can affect people at any age, but the consequences are especially severe when exposure risks intersect with dependency on settings people cannot avoid—such as schools, workplaces, healthcare facilities, public transport, and aged care. Across the lifespan, the central issue remains the same: without safer environments and reasonable adjustments, participation is restricted and disability deepens.
Children and Adolescents
Children with Environmental Sensitivity conditions can be harmed by exposures during critical periods of development, and they often have little control over the environment’s adults place them in. Sensitivities may contribute to neurodevelopmental impacts, learning disruption, and loss of educational access. Fragranced products, cleaning agents, pest treatments, building emissions, and mould in schools can prevent attendance, forcing families into home schooling, reduced participation, or full withdrawal—outcomes that should be treated as an education access and disability accommodation issue.
Adolescents face additional risks as their worlds expand to include workplaces, public transport, social venues, and more technology‑saturated environments. When these settings are not accessible, young people can lose education opportunities, healthcare access, and peer connection—creating preventable isolation and avoidable long‑term disadvantage.
Adults
Adults with Environmental Sensitivity conditions often face a direct pathway from exposure to lost employment. Workplaces, training settings, and services that rely on fragranced products, cleaning chemicals, and poor indoor air quality can become inaccessible. The need for low‑toxicity housing and workplace accommodations creates significant financial strain, and many people report profound losses of professional identity, independence, and community connection.
Older Adults
Ageing can amplify Environmental Sensitivities through reduced resilience, higher care needs, and fewer housing choices. Yet aged care and health services are often among the least accessible environments due to fragranced products, cleaning chemicals, mould, and technology-related exposures. Older adults reported disbelief and inadequate support at a time of increasing vulnerability—an outcome that underscores the need for enforceable accommodation standards in healthcare and aged care.
4.2 Hardships Faced by Individuals with Environmental Sensitivities
Table 20 summarises the main areas where respondents reported being shut out of everyday life. These are not “inconveniences”—they are predictable access barriers created by environments and systems that do not accommodate Environmental Sensitivities. When essential services (healthcare, housing, education, employment, and public spaces) remain saturated with triggers, people are effectively denied safe participation.
Table 20. Challenges faced by individuals with Environmental Sensitivities
| Hardship | Number | Percentage % |
| Medical assistance | 301 | 67.0 |
| Housing | 235 | 52.3 |
| Education | 157 | 35.0 |
| Employment/Income | 345 | 76.8 |
| Social Services | 155 | 34.5 |
| Accessing public places | 305 | 67.9 |
| Relationships/social interactions | 376 | 83.7 |
| Other | 115 | 25.6 |
| Total answered | 449 | 84.2 |
Table 20. Reported types of hardships experienced by respondents with Environmental Sensitivities, expressed as number and percentage of individuals endorsing each category.
The pattern is clear: barriers cluster across multiple life domains, which means people often lose more than one essential support at the same time (for example, housing instability alongside healthcare inaccessibility and employment loss). This compounding burden is exactly why disability recognition and enforceable reasonable adjustments are necessary—so people are not forced to choose between their health and basic participation.
4.2.1 Number of Concurrent Hardships
Counting how many hardship categories each person experiences help show the true scale of disability burden. For many respondents, Environmental Sensitivities affect multiple systems and multiple settings at once—so supports and accommodations must be designed for complexity, not for a single isolated “issue.”
Table 21. Number of Concurrent Hardships reported
| Number of hardships | Number | Percentage % |
| 1 | 36 | 8.0 |
| 2 | 40 | 8.9 |
| 3 | 59 | 13.1 |
| 4 | 68 | 15.1 |
| 5 | 73 | 16.3 |
| 6 | 60 | 13.4 |
| 7 | 55 | 12.2 |
| 8 | 32 | 7.1 |
Table 21. Distribution of the number of hardship categories reported per respondent, indicating cumulative burden among individuals with Environmental Sensitivities.
These results highlight cumulative exclusion: the most common experience is not one barrier, but several. This has direct implications for policy and service design—access standards must be applied consistently across sectors (health, transport, housing, education, and workplaces), because failure in any one sector can collapse a person’s ability to function safely in others.
4.2.2 Additional Hardships Reported
Respondents also reported many additional access barriers, most linked to fragranced products, cleaning chemicals, indoor air quality, mould, and electromagnetic exposures. These barriers are best understood as environmental accessibility failures—conditions that could be substantially reduced through fragrance‑free policies, safer cleaning and building practices, and clear accommodation protocols.
- Public transport: Public transport can be inaccessible due to fragrance exposure, chemical treatments (including insecticides on international flights), and electromagnetic exposures reported by people with EHS. Access requires practical measures such as fragrance‑free guidance, safer product choices, and clear procedures to reduce preventable exposures.
- Shopping: Many respondents cannot safely access shops due to fragranced products, strong cleaning chemicals, and poor ventilation. Creating low‑scent retail environments and reducing unnecessary chemical exposures are straightforward steps that would improve access for a substantial cohort.
- Social isolation: Avoiding triggers can force people into isolation and loneliness, cutting them off from community life and creative participation (e.g., exhibiting art, teaching music, and performance). Some respondents reported being house‑bound or bed‑bound and relying on supports such as air purifiers, oxygen supplementation, and noise‑cancelling headphones—highlighting the need for practical community access measures, not stigma.
- Travel: Travel and accommodation are frequently unsafe due to Wi‑Fi exposure, fragranced cleaning products, and other chemical triggers. Accessibility requires accommodation options that are genuinely low‑scent/low‑chemical, as well as clear disclosure and cleaning standards.
- Daily activities and practical support: Routine tasks (housework, gardening, personal care) can become unsafe when products and environments contain common triggers. Many respondents reported difficulty finding in‑home assistance because support workers may use fragranced products or rely on mobile phones and other devices that can trigger symptoms for people with EHS. Services should treat fragrance‑free and low‑exposure practices as a basic accessibility requirement.
- Medical care: Clinics, hospitals, and aged care facilities are often inaccessible due to fragranced products, cleaning chemicals, and electromagnetic exposures. Respondents also reported dismissal and scepticism from staff and the lack of effective treatments. Healthcare services must adopt clear accessibility protocols so that people are not denied care because of preventable environmental triggers.
- Mental health impacts: Many respondents reported anxiety, depression, and chronic stress linked to ongoing exposure risks and repeated disbelief. Some described extreme psychological distress or trauma‑like symptoms after interactions with family members, healthcare providers, and social services (including Centrelink). These mental health impacts are often secondary to exclusion and should be addressed through both support and environmental harm reduction.
- Financial strain: Respondents described high costs associated with safer products, treatment, and repeated relocation. Moving can be prohibitive yet necessary to avoid triggers such as emissions from nearby infrastructure, new Wi‑Fi installations in schools and public areas, or local chemical pollution. This is a key reason Environmental Sensitivities should be recognised within disability and social support systems.
- Housing: Finding safe housing free from mould, chemical emissions, and electromagnetic exposures is a major access issue. Respondents noted the high cost of remediation and building changes, including addressing mould infestation and emissions from materials such as chipboard (formaldehyde). Housing policy and standards must recognise that environmental access is a health and disability requirement.
Respondents also described everyday exclusion driven by common exposures—such as fragranced products worn by joggers, fragranced cleaning products in public toilets, and barriers to NDIS supports when support workers use fragrances or mobile phones. Similar issues were reported in libraries and other public venues where routine product use makes spaces inaccessible.
Across these accounts, access to public buildings and services emerges as a primary barrier. This reinforces the need for enforceable accessibility standards—particularly fragrance‑free and low‑chemical practices, clean air measures, and clear accommodation pathways—so participation is not contingent on risking health.
Environmental Sensitivities are complex, disabling conditions characterised by extensive multimorbidity and far‑reaching social impacts. The ANRES data show that these conditions are not rare, isolated, or benign. They represent a significant public health and disability issue—one that remains under‑recognised in policy, services, and everyday environments.
What people need is straightforward: recognition, safer environments, and enforceable reasonable adjustments. Practical accommodation across healthcare, housing, employment, education, and public infrastructure can reduce harm, prevent avoidable deterioration, and support equitable participation with dignity.
Section 5.0 The Consequences of Environmental Illnesses
The consequences of Environmental Sensitivities (ES) are far‑reaching chronic illness, disability, restricted participation, and profound loss of quality of life. Many people report ongoing financial hardship, repeated displacement from housing or services, and long‑term reliance on inadequate income supports—often while paying higher costs for safe food, safe products, and safer living conditions.
These outcomes are not inevitable. They are intensified by stigma, inconsistent clinical recognition, and the absence of practical accommodations in everyday environments. Formal recognition and enforceable adjustments can reduce harm, prevent deterioration, and uphold the right to equitable access.
Environmental Sensitivities conditions can result in significant health injury and disability when individuals are exposed to everyday built environments, including healthcare settings, workplaces, housing, education facilities, and public infrastructure. For many, these environments are not neutral spaces—they are sites of harm that worsen symptoms, limit function, and accelerate disability.
In Australia, population‑level exposure to synthetic chemicals, indoor air pollutants, and electromagnetic emissions has increased substantially over recent decades (Bijlsma & Cohen 2016). A significant proportion of man‑made chemicals in use have not been adequately tested for long‑term health effects, while genetic diversity, pre‑existing illness, age, and cumulative exposure histories mean that some individuals experience harm at exposure levels considered “safe” for the general population. These factors contribute to marked inter‑individual variability in susceptibility to environmental injury.
Emerging evidence is showing that Environmental Sensitivities are associated with immune dysregulation, neurological dysfunction, inflammatory processes, and impaired detoxification pathways although the mechanisms are not fully established.
For susceptible individuals, repeated or cumulative exposures can result in escalating intolerance and the development of multiple overlapping chronic conditions. Once established, these conditions often become self‑reinforcing unsafe environments trigger symptoms, symptoms restrict access, and restricted access deepens disability.
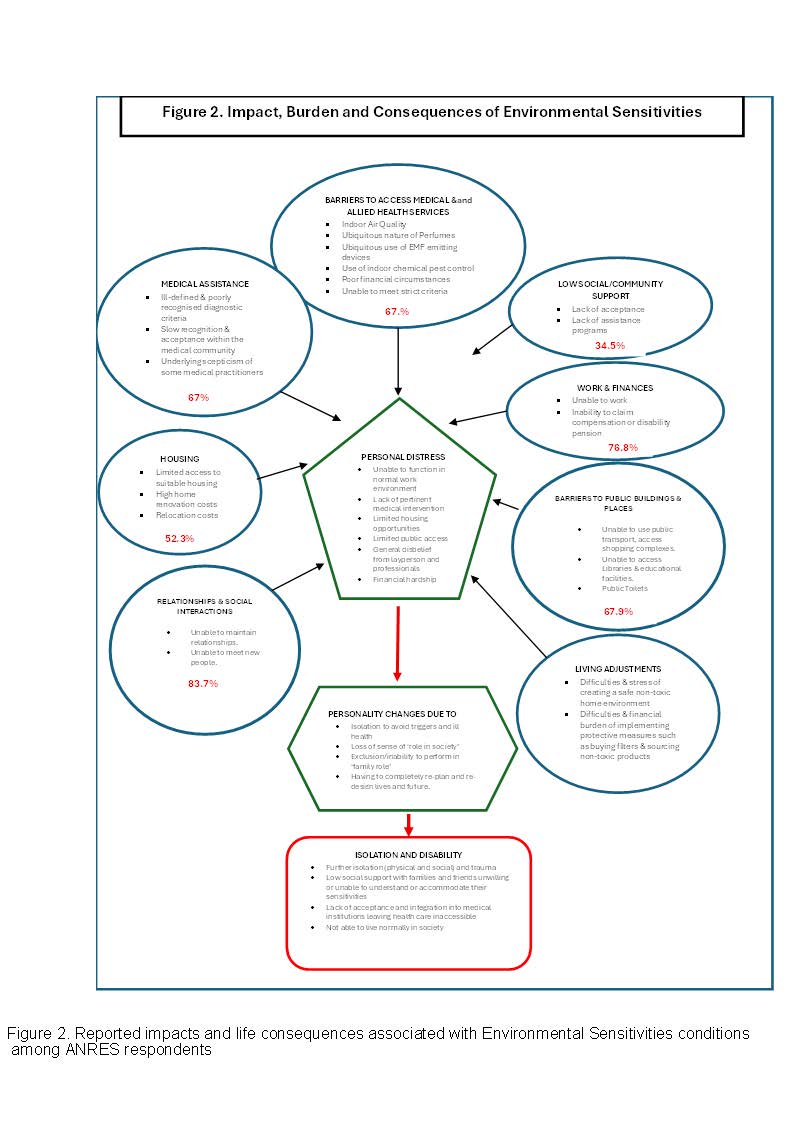
5.1 Impact, Burden, and Disability Consequences
The consequences of Environmental Sensitivity conditions extend far beyond episodic symptoms (Figure 2). Respondents consistently reported pervasive and ongoing impacts across nearly all domains of daily life, including:
- Health deterioration, chronic pain, fatigue, cognitive impairment, and heightened vulnerability to further illness
- Disability and loss of function, particularly where exposure avoidance is not possible
- Employment disruption, loss of income, and forced withdrawal from paid work
- Inaccessible healthcare, including inability to attend clinics or hospitals without triggering illness
- Housing insecurity, driven by the scarcity and cost of safe, low‑toxicity living environments
- Social isolation, relationship strain, and loss of community participation
- Psychological distress, grief, anxiety, and depression secondary to exclusion, disbelief, and chronic stress
These outcomes are not the result of individual coping failure. They reflect systemic environmental accessibility failures that deny people safe participation in essential services and public life.
Educational and clinical resources on Environmental Medicine in Australia are lacking. Toxicant exposure assessment requiring complex areas such as genetics, nutrition and microbiomics are not taught or used/integrated into clinical practice (Bijlsma & Cohen 2018).
Overall Environmental Medicine clinicians feel that educational and clinical resources on Environmental Medicine are lacking in Australia. (Bijlsma & Cohen 2018). This is reflected in overseas papers, where a 2011 US study found that only 30 % of doctors receive formal training about MCS (Gibson & Linderberg 2011). In the Myalgic Encephalomyelitis Association of Ontario (MEAO) study a lack of education and training seen as responsible for negativity, discrimination and neglect (Burstyn & MEAO 2013).
Burstyn and MEAO (2013) found people with Environmental Sensitivity are experiencing socioeconomic disadvantage as demonstrated by high levels of moderate or severe food insecurity and sizeable proportions with low annual household income.
5.2 Living Adjustments and Financial Burden
Many individuals with Environmental Sensitivities must make extensive and ongoing adjustments to daily living to reduce exposure. These commonly include sourcing non‑toxic products, modifying housing, installing air and water filtration, restricting travel, and avoiding public spaces.
Safe housing is not a luxury—it is a medical necessity for many people with Environmental Sensitivities. Limited availability of low‑toxicity, mould‑free, and low‑EMF housing, combined with the high costs of remediation and relocation, pushes many into housing insecurity and, in some cases, homelessness. Unsafe housing can worsen symptoms, trigger relapses, and accelerate disability. A housing response must therefore include practical standards, accessible remediation pathways, and recognition that environmental access is a disability issue.
These adjustments carry significant financial costs that are typically unsupported by health or disability systems. As a result, many people experience long‑term financial strain, repeated relocation, or reliance on inadequate income supports while facing higher daily living expenses simply to maintain basic health and safety.
5.3 Barriers to Healthcare and Support Services
Healthcare and allied health services are frequently inaccessible to people with Environmental Sensitivities due to:
- Fragranced products and cleaning chemicals
- Poor indoor air quality
- Routine pesticide use
- Ubiquitous electromagnetic exposure
- Rigid service models that do not allow environmental accommodations
These barriers mean that some individuals are unable to access medical care even in urgent or emergency situations. Dismissal, disbelief, and lack of practitioner knowledge further compound harm and delay diagnosis and support (Dorion 2007).
Healthcare must be accessible. Yet for many people with Environmental Sensitivities, the very places meant to provide care can trigger illness. Fragranced products, cleaning chemicals, poor indoor air quality, and electromagnetic exposures in medical settings mean some people cannot safely attend clinics or hospitals—even during urgent and emergency situations. This is a preventable access barrier, and it requires clear protocols and environmental accommodations.
Social and community support systems also frequently fail this cohort. Respondents described poor understanding of Environmental Sensitivities, rigid eligibility rules, and repeated dismissal of lived experience. When systems do not recognise environmental access needs, they effectively deny support—and that denial can accelerate isolation, deepen poverty, and worsen health outcomes.
5.4 Social Exclusion, Identity Loss, and Disability Progression
Long‑term exposure avoidance and restricted access to society often result in profound changes to personal identity and social roles. Many individuals report:
- Loss of professional and family roles
- Withdrawal from social and cultural life
- Increased isolation and trauma linked to repeated exposure events and systemic disbelief
- Progressive disability as environments remains inaccessible
Over time, this exclusion can make participation in society severely limited or impossible.
5.5 Summary: Environmental Illness as a Disability Issue
Environmental Sensitivities are not minor sensitivities or lifestyle preferences. They are complex, multisystem conditions that can be severely disabling in environments saturated with chemical, biological, and electromagnetic triggers.
The evidence presented in this report demonstrates that disability is produced not only by illness, but by the failure of environments and systems to accommodate environmental access needs. Without formal recognition, enforceable standards, and practical environmental adjustments, individuals with Environmental Sensitivities are forced to choose between participation and health—often at the cost of both.
Section 6.0 Discussion
This report presents comprehensive evidence from the Australian National Register of Environmental Sensitivities (ANRES) demonstrating that Environmental Sensitivities (ES) are chronic, multimorbid, and frequently disabling conditions with far‑reaching consequences for health, participation, and quality of life. The findings challenge common assumptions that Environmental Sensitivities are rare, isolated, or primarily psychosocial, and instead position them as a significant public health and disability issue that warrants formal recognition and systemic response.
6.1 Environmental Sensitivities as Multisystem and Multimorbid Conditions
A central finding of this analysis is the extent to which Environmental Sensitivities cluster rather than occur in isolation. Most registrants reported multiple co‑existing conditions, often spanning chemical, biological, electromagnetic, neurological, and immune sensitivity domains. Multiple Chemical Sensitivity (MCS), Fragrance Sensitivity, and Food Sensitivity formed a core group of highly overlapping conditions, frequently co‑occurring with CFS/ME, Fibromyalgia, Electromagnetic Hypersensitivity (EHS), Lyme disease, and Biotoxin‑related illness.
This multimorbidity has important implications. First, it explains why exposure risks accumulate rapidly: an environment that is unsafe for one sensitivity is often unsafe across several. Second, it underscores why single‑issue or narrowly framed responses are inadequate. Disability services, healthcare, housing policy, and workplace adjustments must be designed for layered vulnerability rather than for a hypothetical “typical” case.
6.2 Gender, Age, and Cumulative Impact
The ANRES data show a strong gender imbalance, with women disproportionately represented and more likely to report higher levels of multimorbidity. This mirrors patterns seen in other poorly recognised chronic and inflammatory conditions and raises concerns about gendered pathways to diagnostic delay, disbelief, and unmet support.
Age‑related analyses further suggest that Environmental Sensitivities often reflect cumulative environmental injury. Older registrants were more likely to report higher numbers of conditions and longer illness duration, indicating that prolonged exposure, reduced physiological resilience, and limited housing and service options may increase disability severity over time. At the same time, the presence of childhood and early‑onset cases highlights that Environmental Sensitivities can also represent early‑life vulnerability with lifelong consequences when accommodations are not provided.
6.3 Disability Is Shaped by Environment, Not Just Illness
Across the dataset, disability was not determined solely by symptom severity, but by whether environments were accessible. Respondents consistently reported being excluded from healthcare, employment, education, housing, transport, and public spaces due to preventable environmental triggers such as fragrances, cleaning chemicals, mould, and ubiquitous electromagnetic exposure.
This aligns with contemporary disability frameworks, which recognise disability as arising from the interaction between impairment and environment. Inaccessible environments—rather than individual weakness—produced loss of employment, healthcare avoidance, housing instability, social isolation, and psychological distress. These outcomes meet practical definitions of disability regardless of whether legal or administrative recognition currently exists.
6.4 Healthcare Inaccessibility as a Driver of Harm
One of the most concerning findings is that healthcare environments themselves frequently render care inaccessible. Fragranced products, cleaning chemicals, poor indoor air quality, routine pesticide use, and unmitigated electromagnetic exposure prevent some individuals from safely attending clinics or hospitals, even in urgent situations. Dismissal and scepticism further compound harm by delaying diagnosis, undermining trust, and reducing engagement with care.
These barriers represent a systemic failure rather than an unavoidable limitation. The data suggest that relatively straightforward measures—such as fragrance‑free policies, safer cleaning protocols, improved ventilation, and clear accommodation pathways—could substantially reduce exclusion and harm.
6.5 Implications for Policy, Services, and Disability Recognition
Taken together, the findings demonstrate that Environmental Sensitivities are not edge cases but a coherent pattern of environmental disability. The lack of formal recognition exacerbates harm by preventing access to disability supports reasonable adjustments, safe housing pathways, and income assistance that reflects real costs of living safely.
The evidence supports urgent action across multiple domains:
- Disability systems must recognise Environmental Sensitivities as legitimate disabling conditions characterised by environmental access needs.
- Healthcare systems must adopt enforceable accessibility standards to ensure care does not cause harm.
- Housing policy must acknowledge that safe environments are a medical necessity, not a preference.
- Employment and education systems must implement fragrance‑free and low‑exposure practices as accessibility measures.
Failure to act perpetuates avoidable illness progression, financial hardship, and exclusion.
6.6 Strengths, Limitations, and Future Directions
The ANRES dataset provides one of the most detailed national pictures of Environmental Sensitivities in Australia, capturing long illness duration, multimorbidity, and lived impacts across the lifespan. However, as a voluntary registry, it may underrepresent individuals who are severely isolated, digitally excluded, or unaware that environmental factors contribute to their illness.
Future research should focus on longitudinal outcomes, intervention effectiveness, housing and healthcare accessibility models, and the economic costs of exclusion versus accommodation. Continued data collection is essential for informing evidence‑based policy and service reform.
Section 7.0 Conclusion
This discussion reinforces the report’s central conclusion: Environmental Sensitivities represent a significant, under‑recognised public health and disability issue. The harms documented here are not inevitable consequences of illness, but predictable outcomes of environments and systems that have failed to adapt.
Recognition, accommodation, and prevention are not optional—they are necessary to reduce harm, uphold human rights, and enable equitable participation for people living with Environmental Sensitivities.
Overall, this study underscores the pervasive impact of Environmental Sensitivities on the lives of affected individuals. The findings highlight a substantial need for greater recognition, understanding, and practical support to improve quality of life and ensure fair access to essential services. Addressing these challenges requires coordinated action from healthcare providers, policymakers, and society at large to foster a more inclusive and accommodating environment for people living with Environmental Sensitivities. A fundamental shift in attitudes, perceptions, and actions on health and the environment is essential to achieving improved health outcomes, both for individuals and for the broader community.
Appendix: Advocacy Statement on Environmental Sensitivities
Environmental Sensitivities Are a Disability—Recognition Is Long Overdue
Environmental Sensitivities (ES) are disabling conditions that profoundly affect daily life. For those living with Environmental Sensitivities, routine exposures—such as fragranced products, cleaning chemicals, building materials, mould, and electromagnetic fields (EMF)—can trigger serious and sometimes debilitating symptoms.
Despite the severity of these impacts, individuals with Environmental Sensitivities are still largely unrecognised, underserved, and excluded from essential aspects of society. This lack of recognition creates systemic barriers to housing, healthcare, employment, education, and social participation.
This document calls for urgent, coordinated action to recognise Environmental Sensitivities as disabilities and to implement practical, evidence‑informed accommodations that uphold dignity, safety, and human rights.
Key Advocacy Priorities
1. Formal Recognition of Environmental Sensitivities as Disabilities
Environmental Sensitivities must be formally recognised as disabilities across health, housing, employment, and social service systems. Recognition is the foundation for legal protections, reasonable accommodations, and fair access to services. Without it, individuals with Environmental Sensitivities are left invisible and unprotected.
2. Ending Invisibility Through Public Awareness
Environmental Sensitivities are often misunderstood because they are not at once visible. This invisibility leads to disbelief, stigma, and dismissal. Public education initiatives must clearly communicate that Environmental Sensitivities are real, disabling conditions that require accommodation—not debate.
Healthcare professionals, employers, educators, policymakers, and the public all play a role in creating environments that do not exclude people with Environmental Sensitivities).
3. Safe, Accessible Housing Is a Human Right
Safe housing is not optional—it is essential. Individuals with Environmental Sensitivities require housing that is free from chemical, mould, and EMF triggers. The current lack of accessible housing forces many into unsafe living conditions or homelessness.
Governments and housing providers must prioritise:
- Non‑toxic building materials
- Fragrance‑free maintenance practices
- Mould‑safe construction and remediation
- Access to low‑trigger or adaptable housing options
4. Healthcare Access Without Harm
Healthcare should never make a patient sicker. Yet for individuals with Environmental Sensitivities, medical environments often pose serious risks due to fragrances, cleaning chemicals, and EMF exposure.
Advocacy efforts must demand:
- Mandatory training for healthcare providers on Environmental Sensitivities
- Fragrance‑free and low‑trigger healthcare settings
- Safe alternatives for diagnostic and treatment environments
Access to healthcare is meaningless if the environment itself causes harm.
5. Employment With Dignity and Accommodation
People with Environmental Sensitivities want to work and contribute. What they need are reasonable accommodations, not exclusion.
These include:
- Fragrance‑free workplace policies
- Reduced or managed EMF exposure
- Flexible scheduling or remote work options
Inclusive employment practices benefit not only individuals with Environmental Sensitivities, but workplaces.
6. Education Without Exclusion
Students and educators with Environmental Sensitivities are routinely forced out of educational environments due to avoidable triggers. Schools, universities, and training institutions must adopt policies that prioritise accessibility, including fragrance reduction and safer environmental practices.
Education should open doors—not close them.
7. Public Spaces Must Be Accessible to All
Access to public spaces is a cornerstone of social inclusion. Fragrances and unnecessary EMF exposure in public buildings, transport, and services effectively exclude individuals with Environmental Sensitivities from community life.
Simple, low‑cost changes can dramatically improve access and participation.
8. Social Services That Understand and Respond
Social service systems must be equipped to support individuals with Environmental Sensitivities. This includes informed case management, access to proper housing and income supports, and respectful engagement that recognises Environmental Sensitivities as legitimate disabilities.
Strategic Actions for Change
Coordinated advocacy campaigns should centre lived experience, highlight systemic barriers, and call for policy reform. Environmental Sensitivities must be framed as a disability and human rights issue—not a personal inconvenience.
Mandatory education for healthcare professionals is essential. Training must emphasise safety, accommodation, and respect, ensuring that individuals with Environmental Sensitivities receive care without harm or dismissal.
Governments must embed Environmental Sensitivities into disability, housing, health, and workplace legislation. Policy silence perpetuates harm.
Environmental Sensitivities should be formally recognised as a legitimate access and health issue, requiring practical adjustments such as low-toxicity building materials, fragrance-free and well-ventilated public spaces, and clear disclosure of chemicals used in workplaces and services. Embedding these requirements in standards, procurement, and compliance processes would reduce preventable exposure, improve participation, and ensure people are not excluded from housing, employment, education, or healthcare due to avoidable environmental triggers.
Peer support, advocacy networks, and community‑based programs are vital for reducing isolation and amplifying voices that have been ignored for too long.
Continued research and data collection are necessary to inform policy, improve services, and strengthen recognition of Environmental Sensitivities as disabling conditions.
Creating safe environments is achievable. Advocacy should promote:
- Natural, low‑toxicity building materials
- Low‑ or no‑VOC paints and finishes
- Non‑toxic adhesives and sealants
- Natural fibre furnishings
- Solid wood furniture
- HEPA air filtration systems
- EMF shielding where required
These measures are neither extreme nor unreasonable—they are essential accessibility tools.
Section 8.0 References
Allergy, Sensitivity & Environmental Health Association QLD Inc: A survey of individuals with MCS in Australia. ASEHA QLD Inc; 2011.
[https://web.archive.org/web/20180309235911/http:/asehaqld.org.au/index.php/multiple-chemical-sensitivity/aseha-mcs-publication/140-a-survey-of-individuals-with-mcs-in-australia-2011]
Belpomme, D., Campagnac, C. and Irigaray, P., 2015. Reliable disease biomarkers characterizing and identifying electrohypersensitivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Reviews on Environmental Health, 30(4), pp. 251-271.
Bijlsma, N. and Cohen, M.M., 2016. Environmental chemical assessment in clinical practice: unveiling the elephant in the room. International journal of environmental research and public health, 13(2), p.181.
Bijlsma, N. and Cohen, M.M., 2018. Expert clinician’s perspectives on environmental medicine and toxicant assessment in clinical practice. Environmental Health and Preventive Medicine, 23(1), p.19.
Burstyn, V. and MEAO., 2013. Recognition, inclusion and equity–the time is now: Perspectives Of Ontarians living with ES/MCS, ME/CFS and FM. Ontario Centre of Excellence in Environmental Health (OCEEH) [http://recognitioninclusionandequity.org/resources/]
Caccamo, D., Cesareo, E., Mariani, S., Raskovic, D., Ientile, R., Currò, M., Korkina, L. and De Luca, C., 2013. Xenobiotic sensor‐and metabolism‐related gene variants in environmental sensitivity‐related illnesses: a survey on the Italian population. Oxidative Medicine and Cellular Longevity, 831969.
Caress, S.M. and Steinemann, A.C., 2003. A review of a two-phase population study of multiple chemical sensitivities. Environmental health perspectives, 111(12), p.1490.
De Luca, C., Raskovic, D., Pacifico, V., Thai, J.C.S. and Korkina, L., 2011. The search for reliable biomarkers of disease in multiple chemical sensitivity and other environmental intolerances. International journal of environmental research and public health, 8(7), pp. 2770-2797.
Doiron, N.H., 2007. People with environmental sensitivities: Life, identity, and services, Doctoral Thesis in Social Work, University of Toronto.
Fitzgerald, D., 2008. Studies on self-reported multiple chemical sensitivity in South Australia. Environmental Health, 8(3), pp. 33-39.
Genuis, S.J., 2010. Sensitivity-related illness: the escalating pandemic of allergy, food intolerance and chemical sensitivity. Science of the Total Environment, 408(24), pp. 6047-6061.
Genuis, S.J., 2014. Pandemic of idiopathic multimorbidity. Canadian Family Physician, 60(6), pp. 511-514.
Genuis, S.J. and Tymchak, M.G., 2014. Approach to patients with unexplained multimorbidity with sensitivities. Canadian Family Physician, 60(6), pp. 533-538.
Gibson, D.P.R., Cheavens, J. and Warren, M.L., 1996. Chemical sensitivity/chemical injury and life disruption. Women & Therapy, 19(2), pp. 63-79, doi:10.1300/j015v19n02_06.
Gibson, P.R. and Lindberg, A., 2007. Work accommodation for people with multiple chemical sensitivity. Disability & Society, 22(7), pp. 717-732.
Gibson, P.R., 2009. Of the world but not in it: barriers to community access and education for persons with environmental sensitivities. Health Care for Women International, 31(1), pp. 3-16.
Gibson, P.R., Kovach, S. and Lupfer, A., 2015. Unmet health care needs for persons with environmental sensitivity. Journal of multidisciplinary healthcare, 8, pp. 59-66.
Gibson, P.R., White, M.A. and Rice, V.M., 1997. Life satisfaction in persons with invisible disabilities: chemical sensitivity/chemical injury. Poster Delivered at the 21st National Conference, Association for Women in Psychology, (9).
Gibson, P.R., 2014. Life indicators, illness characteristics, and psychosocial concomitants of self-reported multiple chemical sensitivity: A two-year longitudinal study. Journal of Nursing Education and Practice, 4(3), p. 204.
Gibson, P.R. and Lindberg, A., 2011. Physicians′ Perceptions and Practices Regarding Patient Reports of Multiple Chemical Sensitivity. International Scholarly Research Notices, 838930, pp. 1-5.
Gibson, P.R., Sledd, L.G., McEnroe, W.H. and Vos, A.P., 2011. Isolation and lack of access in multiple chemical sensitivity: A qualitative study. Nursing & Health Sciences, 13(3), pp. 232-237.
Halapy, E. and Parlor, M., The Quantitative Data: Environmental Sensitivities/Multiple Chemical Sensitivity (ES/MCS), Fibromyalgia (FM), Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), October 2013 [online]
Hu, H. and Baines, C., 2018. Recent insights into 3 underrecognized conditions: Myalgic encephalomyelitis–chronic fatigue syndrome, fibromyalgia, and environmental sensitivities–multiple chemical sensitivity. Canadian Family Physician, 64(6), pp. 413-415.
Ledoigt, G., Sta, C., Goujon, E., Souguir, D. and El Ferjani, E., 2015. Synergistic health effects between chemical pollutants and electromagnetic fields. Reviews on environmental health, 30(4), pp. 305-309.
Lionetti, F. and Pluess, M., 2024. The role of environmental sensitivity in the experience and processing of emotions: implications for well-being. Philosophical Transactions of the Royal Society B: Biological Sciences, 379(1908).
Miller, C.S., 1997. Toxicant-induced loss of tolerance–an emerging theory of disease?. Environmental Health Perspectives, 105(Suppl 2), p. 445.
Miller, C.S., 1999. Are we on the threshold of a new theory of disease? Toxicant-induced loss of tolerance and its relationship to addiction and abdiction. Toxicology and Industrial Health, 15(3-4), pp. 284-294.
Molot, J., 2013. Chronic complex conditions: Academic and clinical perspectives. Ontario Centre of Excellence in Environmental Health (unpublished); The clinical submission to the Ministry of Health and Long Term Care, supporting the Ontario Centre of Excellence Business Case. [https://johnmolot.files.wordpress.com/2015/12/academic-and-clinical-perspectives-final-october-22-2013.pdf]
Moon, D., 2026. Multiple Chemical Sensitivity (MCS): Genetics, Causes, and Solutions, Genetic Lifehacks. [https://www.geneticlifehacks.com/multiple-chemical-sensitivity-mcs-genetics-causes-and-treatments/] (Accessed: 24 April 2026).
Nordin, S., Köteles, F., Witthöft, M., Van den Bergh, O., Nyback, M.H. and Sainio, M., 2023. Impact of comorbidity on symptomatology in various types of environmental intolerance in a general Swedish and Finnish adult population. Environmental Research, 229, p. 115945.
NSW Department of Health, 2002. The NSW Adult Health Survey. NSW Public Health Bulletin Supplement, p 81-82) https://www.health.nsw.gov.au/phb/Publications/NSW-adult-health-survey-2002.pdf
Sears, M.E., 2007. The medical perspective on environmental sensitivities. Ottawa: Canadian Human Rights Commission. [http://www.chrc-ccdp.gc.ca/sites/default/files/envsensitivity_en_1.pdf]
Shannon, M., Woolf, A. and Goldman, R., 2003. Children’s environmental health: one year in a pediatric environmental health specialty unit. Ambulatory Pediatrics, 3(1), pp. 53-56.
Stein, Y. and Udasin, I.G., 2020. Electromagnetic hypersensitivity (EHS, microwave syndrome)–Review of mechanisms. Environmental research, 186, p. 109445.
Nordin, S., Köteles, F., Witthöft, M., Van den Bergh, O., Nyback, M.H. and Sainio, M., 2023. Impact of comorbidity on symptomatology in various types of environmental intolerance in a general Swedish and Finnish adult population. Environmental Research, 229, p. 115945.
Woolf, A., 2000. A 4-year-old girl with manifestations of multiple chemical sensitivities. Environmental Health Perspectives, 108(12), p.1219.
Zeliger, H.I., 2014. Co-morbidities of environmental diseases: A common cause. Interdisciplinary Toxicology, 7(3), p.117.
Zwillinger, R., 1998. The Dispossessed: Living with Multiple Chemical Sensitivities. Paulden, AZ: The Dispossessed Project. [https://archive.org/details/dispossessedlivi00zwil]
